FOUR RECENT CASES SHOW WHY INDIGENT HEALTH CARE IS HARD TO OBTAIN FOR MONTAGNARD REFUGEES AND HOW COMMUNITY HEALTH WORKERS ARE AN AFFORDABLE SOLUTION FOR TIME-INTENSIVE OUTREACH AND FOLLOW UP
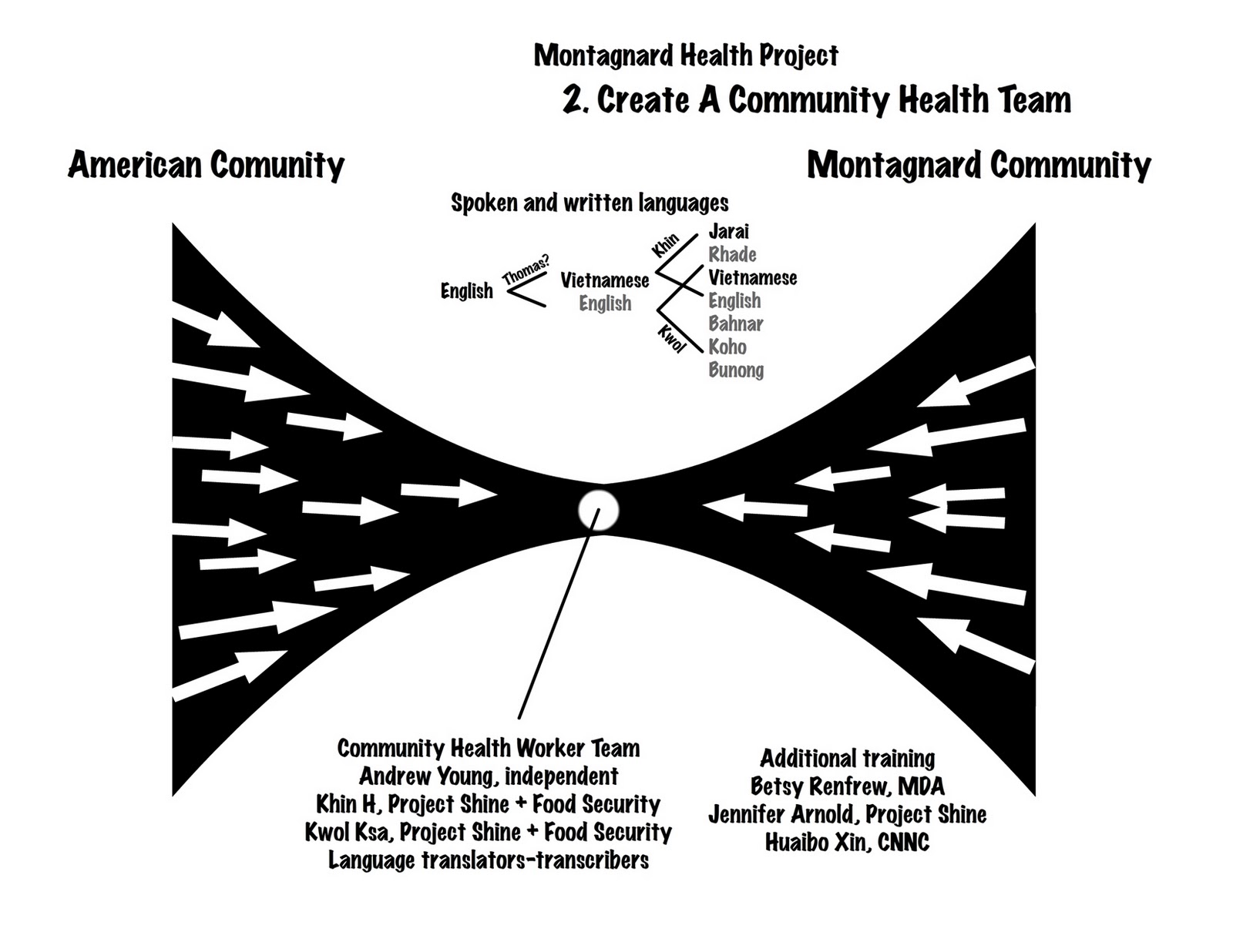
SEE PART 2


SEE PART 2

WORKING WITH MONTAGNARD LAY community health workers, we identified 13 steps to get refugee moms indigent healthcare (the "Orange Card" issued by the Guilford Community Care Network) so they can see a doctor. In Montagnard families, working dads are sometimes covered by employers and children qualify for Medicaid, leaving moms the most vulnerable member. Without health coverage they suffer from illnesses and chronic problems.
Every step presents opportunities for failure. Our lay health workers operate within the cultural constraints of their community. We don't have a steady framework of grants or funding sources to adequately pay them but their liaison skills are critical; they speak all the languages needed to contact families. They are familiar with the qualifying process and can explain it. But the most needy Montagnard families are often preliterate. Financial papers, receipts and junk mail are mixed together. Records are lost or missing.
Recently, we worked with four Montagnard families to get Orange Cards. Our lay health workers — mothers themselves — identified neighbors who hadn't been to a doctor in years. One is in regular pain. Each speaks a different language. Three are preliterate; they do not read their native language. Their English skill is poor. All receive food stamps. If they can find childcare or bus fare, they attend ESOL classes. But in general, the services they receive from local agencies are disconnected and sporadic. It is only through contacts with our lay health workers that we know their plight. We spent the week prepping the women to get their papers together. One got the card, one might get it next week, and two are in limbo.
The first mom is middle aged. Her husband worked but made poverty level (minimum) wages, easily qualifying her for the Orange Card. At the qualifying interview she failed to bring bank statements even though we explained their necessity. The family made it a regular habit to throw them away and because only her husband's name appeared on the statement, we couldn't go to the bank and get copies.
The second mom came from a very troubled home. She looks like she's sixty but her ID states she's in her early 50s. She has several grown kids back in Vietnam and lots of grandchildren there, too. Several months ago we tried to get her an Orange Card and failed. Then we tried again at a health fair. Her paper work was good and her son accompanied her to verify his wages. But she never got her card. By our third try her family's circumstances had changed. Her husband was out of jail but unemployed. The son was no longer being paid under the table by his employer. He had check stubs — proof of income — but now he was working out of state. He'd be back in another week, maybe. In the meantime, our second mom suffers from chronic pain.
The third mom is from a young family. The husband works sporadically and is now out of town. We'd like to get him to verify his wages (again, they're poverty level). The husband doesn't have a great reputation but we're trying to help his wife, not him. If we can get records of his recent wages she can get an Orange Card. We have asked a community leader for additional assistance.
The fourth mom is middle aged. Her husband is elderly but works part time. She is well liked by people in her community and has rudimentary writing skills. She has all her paper work in order and receives her Orange Card. Our lay health workers will follow up and schedule her first doctor's appointment at Healthserve with a call next week.